Last updated on June 23, 2013
Why does female genital cutting (FGC) persist in certain places while has declined elsewhere? Using survey data from the Gambia, we study an important aspect of the persistence of FGC, namely the relationship between (i) whether a woman has undergone FGC and (ii) her support for the practice. Our data exhibit sufficient intrahousehold variation in both FGC status and in support for the practice to allow controlling for unobserved heterogeneity between households. First, our results suggest that a woman who has undergone FGC 40 percentage points more likely to be in favor of the practice, from a baseline likelihood of 40%. Second, our findings indicate that 85% of the relationship between whether a woman has undergone FGC and her support for the practice can be attributed to individual- or household-level factors, but that only 15% of that relationship can be explained by factors at the village level or beyond. This suggests that village-wide pledges against FGC, though they have worked well in neighboring Senegal, are unlikely to be effective in the Gambia. Rather, policies aimed at eliminating FGC in this context should instead target individuals and households if they are to be effective.
That’s the abstract of my most recent working paper (see here for the RepEc version, and here for the SSRN version), “All in the Family: Explaining the Persistence of Female Genital Cutting in The Gambia,” which my former Masters student Tara Steinmetz (who was a Peace Corps volunteer in The Gambia) and I have been working on for quite some time. A previous version had been circulated for the Midwest International Economic Development Conference, but this one is considerably improved. As with any working paper, the caveat that these results have not yet been through the peer-review process applies.
As the abstract above indicates, what is really nice about our data is that they exhibit enough within-household variation in FGC to allow holding household-level factors constant for the women within a given household. This then allows quantifying the contribution of each level of variation — individual, household, village, and district — to the persistence of FGC, defined here as the relationship between a woman having undergone FGC and whether she supports the practice.
Our findings suggest that in The Gambia:
- The average woman aged 15-49 is 40% likely to support FGC. Having experienced FGC, however, makes a woman twice as likely to support FGC, i.e., it increases the likelihood that she will be in favor of FGC to about 80%.
- About 85% of FGC persistence can be explained by individual- and household-level factors, and only 15% of it can be explained by factors at or beyond the village level (e.g., district, region, etc.) The following figure illustrates that point.
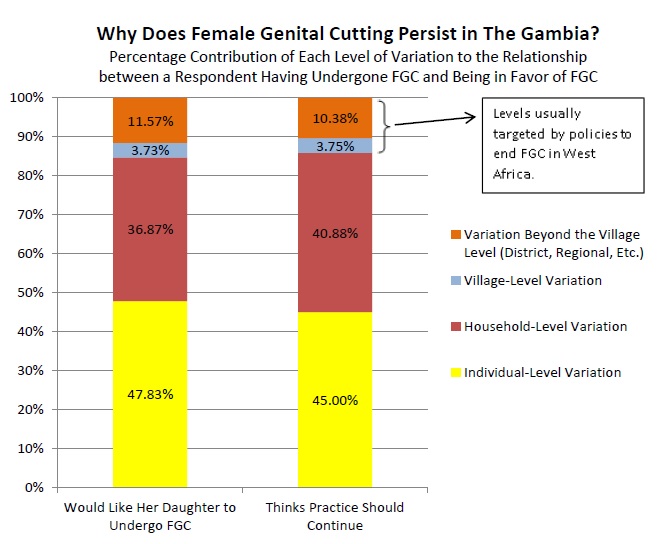
This does not bode well for some of the policies that have so far been used to eliminate FGC in West Africa. In Senegal, which encompasses almost all of The Gambia, village-wide pledges to stop practicing FGC have seemingly been effective in phasing out the practice; similar village-wide pledges had previously been effective against foot-binding in China (see Mackie’s fascinating 1996 American Sociological Review article). Given our results, however, there is little hope that similar village-level pledges will work to phase out FGC in The Gambia: if 85% of the action occurs at the individual and household levels, targeting the village level does not seem like the most promising idea.
Really interesting paper- and a good translation of the findings into something that policy makers can easily digest and hopefully apply.
Thanks, Natalie. We’ve worked very hard to make sure that this was intelligible to nonspecialists, so that is a very nice compliment.
Marc – I don’t know if I’ve recommended it to you before, but have you read Kwame Anthony Appiah’s _The Honor Code_? There’s quite a bit in there about footbinding and its eventual decline. Given the findings on marriage in the conclusion of your paper (the Wagner cite), I think it would be an interesting read for you.
I’m not sure you had, Kim, but it is now on my wish list thanks to your recommendation.